
Gastroenterology Center offers diagnosis and advance treatments for liver and digestive tract diseases including:
• Abdominal Pain
• Heartburn /
Gastroesophageal Reflux Disease (GERD)
• Difficult or Painful Swallowing
• Ulcers
• Nausea and Vomiting
• Irritable Bowel Syndrome (IBS)
• Crohn's Disease
• Ulcerative Colitis
• Gas / Bloating
• Constipation
• Diarrhea
• Fecal Incontinence
• Rectal Bleeding
• Hemorrhoids
• Colon Diseases
• Liver Diseases
• Pancreatic Diseases
• Gallbladder Diseases
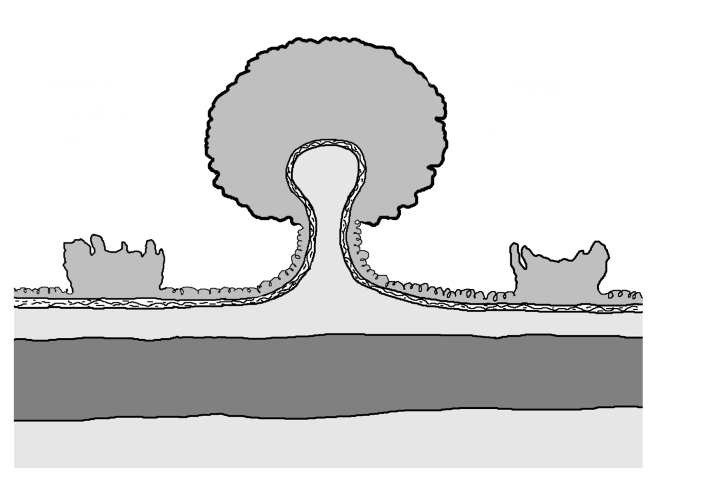
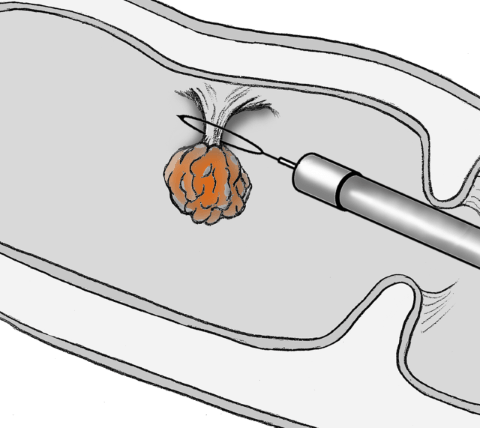
Colon cancer is the third most common cancer and the second highest cancer killer in America, but in its early stages, it is highly treatable. Furthermore, removing colon polyp during a colonoscopy prevents colon cancer from developing.
Colon cancer symptoms:
• bleeding from the rectum
• blood in or on the stool
• changes in bowel patterns
• diarrhea or constipation
• abdominal pain
You are at risk for developing colon cancer if you are 45 years or older. You are at increased risk if you have a personal or family history of benign colorectal polyp, ulcerative colitis Crohn's Disease, or a family history of colon cancer. Schedule a colonoscopy to screen for cancer and remove any polyp before cancer develops.
GERD, or acid reflux, occurs when stomach acid backs up into the esophagus. When the lower sphincter muscle between the stomach and esophagus is weakened or too relaxed, it can allow stomach acid to move into the esophagus.
GERD symptoms include:
• heartburn
• chest pain
• hoarseness
• belching or burping
• difficult or painful swallowing
• chronic cough and wheezing
• back-up of stomach contents into the throat
Irritable Bowel Syndrome, or IBS, is real and affects an estimated 35 million Americans. Although no cure is currently available, there are ways to treat and cope with its daily challenges.
IBS symptoms include:
• abdominal pain
• abdominal discomfort
• alternating bowel habits
• gas
• bloating
• Urgency to have a bowel movement
Anorectal manometry is a test performed to evaluate patients with constipation or fecal incontinence. This test measures the pressures of the anal sphincter muscles, the sensation in the rectum, and the neural reflexes that are needed for normal bowel movements. The test takes about 30 minutes and done in the clinic. It is painless and can help identify the cause of the constipation and fecal incontinence.
Hemorrhoids refer to a condition in which veins around the anus or lower rectum are swollen and inflamed causing rectal bleeding, skin irritation, itching, painful swelling or a hard lump around the anus. When traditional medical treatment is ineffective. Office procedures including Banding or Infrared technologies will relief the hemorrhoids symptoms quickly. No preparation or anesthesia needed and almost pain-free.
Capsule endoscopy is a procedure that uses a tiny wireless camera to take pictures of your digestive tract. The camera sits inside a vitamin-sized capsule that you swallow. As the capsule travels through your digestive tract, the camera takes thousands of pictures that are transmitted to a recorder you wear on a belt around your waist or over your shoulder.
Capsule endoscopy helps doctors see inside your small intestine — an area that isn't easily reached with conventional endoscopy. Capsule endoscopy can be used by adults and by children who can swallow the capsule. The procedure is usually started in a doctor's office.
Fecal microbiota transplantation (FMT), often referred to as ‘fecal transplant’, is rapidly becoming accepted as a viable, safe, and effective treatment for recurrent Clostridium difficile infection (CDI). CDI is a frequent nosocomial illness, and identified as the pathological agent in 10–20% of cases of antibiotic-associated diarrhea, and as high as 50% in epidemic outbreaks. [read more ..]
The New Patient Registration Forms, that can be downloaded from the link below, are provided for your convenience and will save you time at your first visit. Please print these forms, complete, and bring with you.
- To schedule a visit, or for questions, please call our office at 817-551-6161.
- Contact your insurance company prior to your visit to verify your coverage and get understanding of your cost sharing charges including copay, coinsurance and deductible.
- A referral must be obtained from your Primary Care Physician (PCP) before your first visit, If required by your insurance policy (Most HMOs and other plans).
Dr. Mike Bismar considers his greatest professional accomplishment to be the trust that his patients place in him. That trust is built on the time that Dr. Bismar spends listening to each patient and focusing on their needs. High-level technology and advanced treatments are tools to be used only after the physician and patient have thoroughly communicated and all the patient's concerns have been addressed.
At the Gastroenterology Center, Dr. Mike Bismar combines his extensive training at the world-renowned MD Anderson Cancer Center with years of patient care experience to provide excellent care. Board certified in both internal medicine and gastroenterology by the American Board of Internal Medicine and Gastroenterology, Dr. Bismar has the knowledge, compassion and sophisticated technology to diagnose and treat conditions of the liver and digestive system.
Training
Gastroenterology Fellowship
• University of Texas Medical School at Houston
• MD Anderson Cancer Center, Houston
Internal Medicine Residency
• University of Texas Medical Branch at Galveston
Education
Medical School
• University of Texas Medical School at Houston
Undergraduate
• Bachelor of Science in Applied Mathematics, University of Houston-Downtown, Texas. summa cum laude

You are important to us. Providing quality, safe care to every patient every time is at the heart of what we do. That's why our staff, clinical and non-clinical alike, is fully committed to excellent care and a positive patient experience. At the Gastroenterology Center, we are always looking for ways to improve your care. We are on the cutting-edge best practices and participate in national endeavors that promote quality and patient safety. We strive to be the best we can be to ensure the best possible outcome.

"Overall, a very pleasant experince. Dr. Bismar available to talk about the procedure."
"Overall, the experience was very good. Nurses were efficient, friendly, knowledgable. Dr. Bismar very professional."
"Everyone involved in my procedure were carring, patient with me and understanding with me and cared for me as if I were family. it was particularly comforting to meet those who would be w/me wduring the procedure. Dr. Bismar was concerned by what he discovered from procedure, so it is very comforting to know he truely cares for me as on of his patients."
These FAQs are provided for informational purposes only and should not be considered medical advice or guidance for at-home treatment. Portions of this content have been adapted from the American Cancer Society and other reputable sources.
If your question is not answered below, please contact our office at 817-551-6161 for further assistance.
Facts and Figures about Colon Cancer (AKA Colorectal Cancer or CRC)
Data source: American Cancer Society | Colorectal Cancer Facts & Figures.
We'd love to hear from you! Please call us to schedule an appointment, or if you have any question or request concerning our services, or information on this website.
 If you have an emergency, call 911
If you have an emergency, call 911

Texas Health Huguley Hospital
Medical Office Building 3
11801 South Freeway,
Suite 140
Burleson, Texas 76028